One of the most successful meetings of the last decade has been the Manchester Home Dialysis conference. Run under the stewardship of Sandip Mitra, for the last 9 years it has been the event to attend for patients, carers, industry and clinical teams with an interest in supporting dialysis at home.
And that support is needed. Despite the view that the UK underachieves in getting people onto home dialysis, be that peritoneal or haemodialysis, and the excellence of the meeting, progress remains slow. Low numbers at home and huge variation between centres remain at the heart of the issue. Why?
The why as it turns out is very difficult to nail down. Certainly, clinicians show a strong preference for home therapies when asked the question – especially if directed as a personal choice – as confirmed in BMC Nephrol. (2014 Jan 15;15:16. Nephrologists’ perspectives on dialysis treatment: results of an international survey. Fluck RJ, Fouque D, Lockridge RS Jr). Even a proportion of frail individuals might be suitable with the right support. Yet variation persists. The latest UK Renal Registry report has a range of home dialysis rates from 0-40% between centres in the UK. So what might be the real barriers?
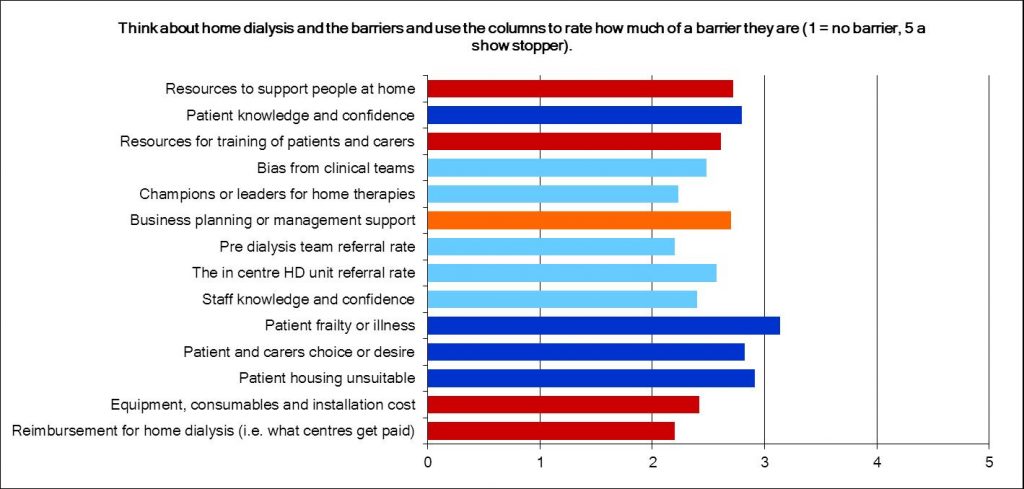
At the 2016 conference, attendees and then the general nephrology community, responded to an online survey. Covering a broad range of expertise and clinical role, 185 individuals kindly completed the survey. The bar chart show the responses to one of the questions – patient factors in blue, resource factors in red and service factors in orange. A common discussion point is about finance, but in terms of barriers it was not felt to be the principle barrier. Patient factors were identified as a leading factor (in blue) followed by resources and service issues including staff knowledge. Business planning and resources were the biggest identified issues in those categories. What was interesting was that in centres with high leadership values organisational barriers and staff barrier ratings all fell significantly, from scores of 2.5 – 3.0 down to 2.0 – 2.2. This implies that good leadership is part of the solution to overcoming these problems. In contrast the perception of patient factors as barriers did not change. So, where there is a will there is a way! What can be done?
A realisation that the barriers are internal to the service – around leadership and knowledge – is quite useful. It tells us that the organisational system around commissioning and pricing is not the issue, it is how multiprofessional teams acquire the skills, knowledge and confidence to support people to undertake a home dialysis treatment. It is about the leadership and vision that gives the permission to change whilst providing some challenge to the way care is delivered. Simple words, simple ideas, not always easy to deliver. So, what is next?
KQuIP is committed to supporting a national programme of improvement for home dialysis. Working with networks of providers, a project structure will be developed by KQuIP, the UK Renal Registry, the Home Dialysis Conference experts and most importantly, you. Work is underway to design the project, find the funding and make a change. Be part of it and give us your thoughts. In the meantime: THINK HOME DIALYSIS!

Richard Fluck
Richard is Consultant Nephrologist and Director of the Renal Unit at Derby Teaching Hospitals NHS Foundation Trust, Chair of the Think Kidneys Programme Board and Co-Chair of the Transforming Participation in Chronic Kidney Disease Programme.
Richard trained at Trinity Hall, Cambridge and the London Hospital Medical College, qualifying in 1985. His early training was in the East London area before he moved into research at St Bartholomew’s Hospital. Richard was appointed a British Heart Foundation Fellow to explore the link between cardiovascular disease, calcium signalling and abnormalities of calcium metabolism in chronic kidney disease. He returned to the Royal London Hospital as lecturer and honorary senior registrar in nephrology, before being appointed as a single handed nephrologist at Derby in 1996.
In 2013 Richard was appointed National Clinical Director for Renal for a three year tenure and has also chaired the Kidney Alliance as well as being President of the British Renal Society. Richard’s special interests are in chronic kidney disease, acute kidney injury, home dialysis therapies, reducing infection in dialysis patients and vascular access.
Richard describes himself as a ‘gadget geek’ and struggles to manage without technology when he’s camping. Away from work music is important to Richard – he plays guitar (and, we’ve heard tell, the ukulele and that he once played in an Abba tribute band, listens to Genesis. His favourite place to visit is the Larmer Tree Festival. He’s also a keen reader and theatre lover.
There are a few other things it might be useful to know about Richard. He qualified as a marksman for the British Army, nearly fell out of a helicopter over Salisbury Plain, drove a 50 ton tank that had no brakes, and during his time in Cambridge rode a bike only three times, all of which ended in injury! Given you’re a keen marathon runner Richard we’d like to suggest you’re safest on two legs! We’ve also heard he goes to Derby County matches, but isn’t a supporter – just takes his son along…….yeah right……